May 31, 2026
When It Comes to Health, Some People Are Born Lucky. Gene Editing May Finally Change That
For years, patients have criticized Big Pharma for selling them drugs they have to take for life. Eli Lilly may be writing a different story. A gene editing treatment that could mean a lifetime free from heart medication.
New Phase 1b clinical trial data from Lilly’s VERVE-102 program suggests that a single dose of a base-editing medicine can permanently silence the gene responsible for high LDL cholesterol, producing durable reductions that persist up to 18 months after treatment. The technology is early-stage and the evidence is preliminary, but the underlying biology is some of the most compelling in cardiovascular and longevity medicine today.

The Gene Variant That Changed Cardiology
In the early 2000s, researchers studying a large database of genetic sequences made an observation that would quietly reshape cardiovascular medicine. A small subset of people, scattered across different populations, carried mutations in a gene called PCSK9 (proprotein convertase subtilisin/kexin type 9) that rendered it largely inactive. These individuals had unusually low LDL cholesterol across their entire lifetimes. And they were, by almost every measure, completely fine.
No developmental problems. No unusual illness. Just low LDL and, notably, dramatically lower rates of coronary heart disease over the course of their lives. In some studies, PCSK9 loss-of-function carriers showed as much as an 88 percent reduction in lifetime coronary heart disease risk compared to non-carriers.
This mattered for a reason that extended beyond the carriers themselves. Because these individuals represented a decades-long natural human experiment, their existence provided safety evidence that nobody had to design or fund. People can live an entire healthy life with PCSK9 substantially or completely silenced. That finding became the scientific rationale for an entire class of drugs, and now it is the rationale for something more ambitious: editing the gene itself.
What PCSK9 Actually Does in the Liver
PCSK9 is a protein produced primarily by the liver. Its normal function is to bind to LDL receptors on liver cell surfaces and flag them for destruction. Fewer receptors means less machinery available to clear LDL from the bloodstream, so circulating LDL rises. The gene has a plausible evolutionary rationale, but in modern humans eating modern diets and living modern lifespans, its activity tends to work against cardiovascular health.
Current PCSK9 inhibitor drugs, injectable antibody therapies approved by the FDA, work by blocking the PCSK9 protein after it is produced. They are effective at reducing LDL, sometimes dramatically so. The limitation is mechanical: the antibody wears off. Stop taking the drug and PCSK9 activity returns, LDL rises again, and the protective effect disappears. Patients with familial hypercholesterolemia (FH), a genetic condition characterized by lifelong LDL elevation affecting roughly one in 200 to 250 people, may require these injections indefinitely.
The question VERVE-102 is designed to answer is whether you can address the problem upstream, at the level of the gene, rather than managing the protein output continuously.
Base Editing: A More Precise Tool Than CRISPR
Most people who follow developments in gene therapy have heard of CRISPR. CRISPR-Cas9 works by cutting both strands of DNA at a targeted location and letting the cell’s natural repair machinery stitch things back together. The approach is powerful and has produced the first approved gene therapies for conditions like sickle cell disease, but it has limitations: the repair process is imprecise at the edges, and double-strand breaks introduce risks of unintended genomic rearrangements. (For a primer on how CRISPR works, the Innovative Genomics Institute has a clear, accessible overview.)
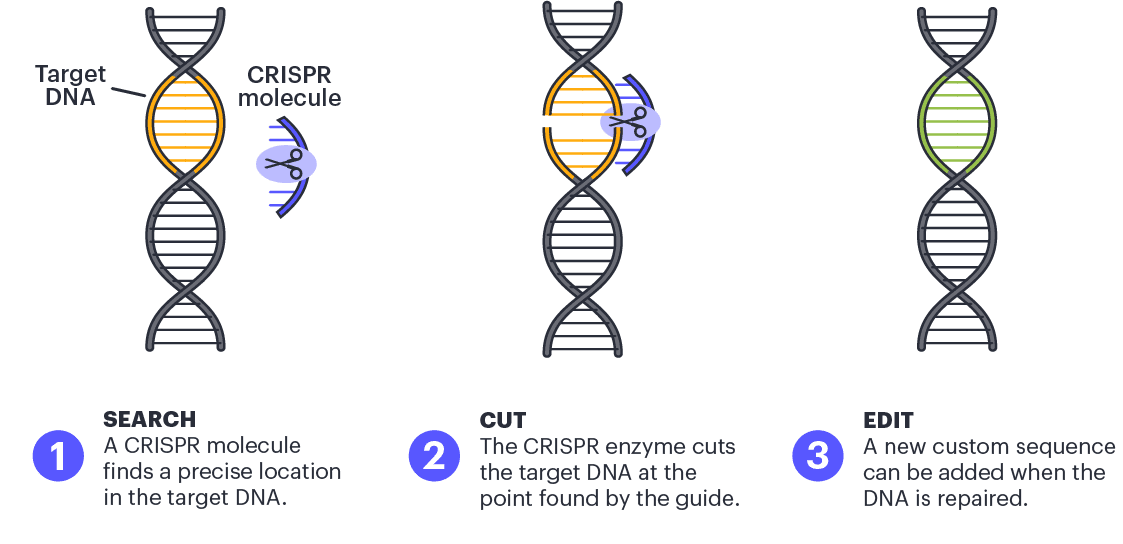
Base editing is a more recent and more precise tool. Rather than cutting DNA, a base editor chemically converts one DNA letter to another directly, without breaking either strand of the double helix. Think of CRISPR as scissors and base editing as a pencil eraser with a built-in replacement. The edit is made at a single nucleotide position, which is the level of change required for many of the most clinically relevant genetic variants.

VERVE-102 uses an adenine base editor, which converts an adenine (A) to an inosine, read by the cell as a guanine (G). Paired with a guide RNA that directs the editor to the PCSK9 gene in liver cells, the medicine makes a single-letter change that converts a functional PCSK9 gene into one that closely mimics the naturally occurring loss-of-function variant. The editor is packaged with the guide RNA inside a lipid nanoparticle engineered to target hepatocytes specifically, and administered as a single intravenous infusion over approximately four hours.
Once the edit is made in a liver cell, it is permanent in that cell and in any daughter cells produced when the cell divides. The liver continues regenerating hepatocytes carrying the edited gene. No ongoing drug is required.
What the Phase 1b Heart-2 Trial Data Showed
The Heart-2 study enrolled 35 adults with heterozygous familial hypercholesterolemia or premature coronary artery disease, a population for whom standard lipid-lowering therapy has not achieved sufficient control. Participants received a single infusion across six ascending dose cohorts and were followed for a minimum of 28 days, with a subset followed for up to 18 months.
Across all dose levels, PCSK9 reductions were dose-dependent and LDL reductions followed. At the highest evaluated dose of 1.0 mg/kg, mean PCSK9 levels fell by 88 percent and LDL-C fell by 62 percent. These reductions were sustained throughout the follow-up period. No treatment-related serious adverse events were reported, no dose-limiting toxicities were observed, and no participant withdrew from the study.
Results were presented as a late-breaking oral session at the European Atherosclerosis Society Congress and simultaneously published in The New England Journal of Medicine. Lilly plans to begin enrolling a Phase 2 study before the end of 2026.
For the complete data, Lilly's official announcement is available here.
Why PCSK9 Silencing May Matter Beyond Cholesterol
Cardiovascular disease is the obvious frame for these results, and the most immediate one. But the implications of PCSK9 loss-of-function extend further, and that extension is where the science becomes relevant to a broader longevity conversation.
Large-scale genetic studies examining people who carry natural PCSK9 loss-of-function variants have found protective associations that go beyond coronary artery disease and stroke. Genetically reduced PCSK9 function has been associated with lower rates of peripheral artery disease and abdominal aortic aneurysm. More intriguingly, one analysis of more than 312,000 individuals found a statistically significant association between genetically lower PCSK9 activity and reduced risk of dementia.
The dementia finding requires careful handling. It is genetic association data, not a randomized trial, and it does not prove causation. What it does suggest is that the vascular contribution to cognitive decline, a relationship that has been increasingly well-characterized in the research literature, may be partially modifiable through sustained LDL management over a lifetime. A drug taken monthly for cardiovascular benefit is not the same as a gene that has been quietly running at reduced output since birth. Whether the results of a lifetime of naturally lower PCSK9 activity can be replicated by a single edit in midlife is one of the central unanswered questions in this research program.
This is not a peptide therapy, and AIRA does not offer gene editing. But it sits squarely in the larger question that increasingly defines the frontier of longevity medicine: what does it mean to intervene at the root cause of biological aging risk, rather than managing its downstream symptoms? PCSK9 silencing is one of the most scientifically credible proposals yet made for doing exactly that in the cardiovascular system.
What the Evidence Does Not Yet Show
Heart-2 enrolled 35 people. The median follow-up at the data cutoff was approximately nine months, with 15 participants followed for at least one year. These are early human data from a single-ascending-dose study, which is explicitly designed to test safety and tolerability first, pharmacodynamic response second. The numbers are not large enough and the follow-up is not long enough to draw conclusions about hard cardiovascular outcomes.
Phase 2 enrollment, announced for later this year, will expand the participant population and provide more robust data on durability, dose optimization, and safety in a broader group. Participants in Heart-2 are expected to enroll in a long-term follow-up study lasting up to 15 years, which will eventually provide the kind of evidence needed to evaluate whether sustained PCSK9 silencing via base editing actually reduces heart attacks and strokes at the level that genetic epidemiology would predict.
Open questions also remain about the base editing technology itself. Off-target editing, the risk that the adenine base editor converts unintended nucleotides elsewhere in the genome, is an active area of scrutiny across the field. The lipid nanoparticle delivery technology is liver-specific by design, which reduces but does not eliminate the possibility of off-target activity in other tissues. Early human data from Heart-2 did not reveal safety signals, but the follow-up required to characterize rare or long-latency effects is measured in years, not months.
The most precise statement the current evidence supports is this: in a small group of high-risk adults, a single dose of VERVE-102 produced large and durable reductions in PCSK9 and LDL-C, with no serious adverse events, for up to 18 months. That is a meaningful result. What it eventually becomes depends on trials that have not yet been completed.
References
CRISPR image from Innovative Genomics Institute







